Gerald H. Smith, D.D.S. Langhorne, Pennsylvania and
Heather Ashton, LCT Fletcher, North Carolina
Past orthodontic research by Schwarze, “Expansion and Relapse in long Follow-Up Studies”, concluded “… that orthodontically induced transverse sizes of the dental arches are very unstable.” The article further stated that, “the majority of patients showed a decrease of the transverse molar and canine distance from the end of treatment to the follow-up examination.” Also emphasized was the fact that “prolonged retention periods do not prevent relapses”. These findings are based on orthodontic techniques that focus on movement of teeth and maxillary expansion without regard for existing cranial base and cranial bone distortions.
Advanced clinical research by Dr. Darick Nordstrom and the authors have uncovered one of the mechanisms that cause orthodontic relapse and why the traditional orthodontic/orthopedic model has failed. Many functional and traditional orthodontists accept the concept that a corrected dentition has a greater probability of remaining stable when the forces of the dental musculature are in a state of harmony. The advanced paradigm expands that concept to include harmony of the cranial mechanism (28 cranial bones and dural membrane system).
When the foundation of a house is crooked so is every doorway, floor or other component that is attached to the faulty base. The stomatognathic system is no different. Cranial balance must first be achieved in order to neutralize the abnormal forces generated by an imbalance of the cranial dura, muscles, ligaments and fascia that directly affect the mandibular condyles. pre-maxilla, maxillae and indirectly the teeth housed in these structures. These abnormal forces act to rebound the cranial lesions (torsions, side bends, compression, etc.) and attached musculature to their abnormal pre-treatment position. In the majority of cases expansion and/or “correct” tooth alignment is incapable of overcoming the greater rebound forces generated by the living tissue. These abnormal forces are programmed into the musculature and functionally deformed osseous structures just like the memory patterns in a orthodontic wire. It is for this reason that over 50% of unilateral posterior crossbites and a higher percentage of transverse expansion cases fail.
The cranium is a dynamic functional unit with an intricate biofeedback mechanism. Internally, the dural membrane system, with its diffuse sensory innervation from the trigeminal nerve, has extensive attachment to the surfaces of the primary cranial bones (sphenoid, frontal, temporals, occiput and parietals). Externally, the multitude of muscles, with their motor and sensory innervation form an ingenious mechanical arrangement with the one hundred plus cranial sutures that helps release tensions in the skull. Balance of this architectural marvel is effected by an elaborate proprioceptor system that constantly feeds information on the changes that are taking place.
A cephalometric analysis is a vital guide in evaluating orthodontic treatment and helps the clinician assess facial growth patterns, treatment prognosis and proper placement of elastics. A cranial palpatory examination is just as important in the evaluation process. Evaluating four simple indicators will alert the clinician to the presence of the potential orthodontic relapse factors. The greater the stress pattern within the cranium the greater the influence the relapse factors will play out when retention is terminated. This is the reason why many orthodontists leave bonded lingual retention wires or instruct patients to wear retainers forever. A more accurate means of predictability for post orthodontic relapse is now available to every clinician. A simplified technique has been developed that will help the clinician assess the relapse factors within 60 seconds or less.
When applied stress goes beyond the physical characteristics of a mechanical system’s ability to adapt, that system will dissipate the inherent stress by deformation. Birthing trauma, forceps delivery, physical trauma to the head, routinely sleeping face down by an infant, rapid palatal expansion, four bicuspid extraction-retraction orthodontics, ligamentous, fascial, muscular and/or dural tensions will all have the ability to deform the skull. Excess compressive forces directed toward the facial bones will cause the skull’s foundation, maxillae, sphenobasilar symphysis (sphenoid-occiput junction), to twist in a sagittal plane, bend and/or rotate to one side in a transverse plane, shift the sphenoid or occiput superiorly or inferiorly or laterally in order to release the tension. The other cranial bones will compensate by moving either inward or outward to adjust to the changes in the foundation. Invariably, it is these forces which clinically manifest themselves as a narrowed anterior maxillae (decreased intercanine width) with a restricted pre-maxillae and accompanying crowding of the four anterior incisors and posterior teeth. Transverse or sagittal expansion which does not permit or address correction of these cranial distortions will often result in orthodontic relapse in a high percentage of cases.
It has been the clinical experience of Dr. Nordstrom, the authors and those dentists who have used the ALF appliances to correct deficient intercanine width, that expansion is achieved with minimal or no relapse. The success of reducing relapse is attributed to using the four indicators as a guide during orthopedic treatment. The ALF appliance’s physiologic design employs a specially designed anterior omega loop. This loop applies a light continuous force which releases the pre-maxilla, the fourteen facial bones and allows the cranial stress patterns to dissipate thus establishing a dental foundation that is in a neutral position. The ALF is the only lightwire functional appliance that offers this feature.
As noted in the orthodontic literature, unilateral posterior crossbite is a relatively common dental malocclusion. This abnormality is already prevalent in the deciduous and mixed dentitions. Because of the great potential for a unilateral posterior crossbite to lead to a skeletal deformity its correction at an early age is highly recommended.
A recent study by Brin1, et al verifies and corroborates other studies 2,3,4 that reveal maxillary arch widening by at least 1.5 mm but that 50% of the unilateral posterior cross bites relapse following lateral expansion.
Once again the orthodontic/orthopedic treatment in these studies never considered the distortion patterns of the cranial base and other cranial bones that cause orthodontic relapse. If these factors are never evaluated and addressed, all clinical research studies that employ the same conventional philosophy and treatment concepts will replicate the results and reinforce the practitioner’s belief that relapse will occur 50% of the time.
Case Study: Retreatment of a failed unilateral posterior crossbite. Christina G. is a 15 and three quarter year old Caucasian female that presented with the following chief complaints:
- Failed orthodontic treatment to correct a unilateral right posterior crossbite.
- Chronic fatigue
- Upper cervical instability
- Pelvic instability
- Bilateral Pains behind the eyes
- Occasion ringing in the ears
Past Dental History: The patient underwent non-extraction Crozat and conventional orthodontic fixed appliances. The right posterior cross bite never corrected with treatment.
Cranial Evaluation of Relapse Factors (*):
- * Sphenoid: high on the right
- * Temporal bone: internal rotation on left
- * Amplitude: greater on right side
- * SBS (Sphenobasilar Symphysis): right side bend lesion
- Reversed sphenobasilar mechanism
- Right half of the maxillae internal rotation
Dental Findings:
- Pre-maxillae restricted
- Maxillary intercanine arch deficiency
- Right side maxillary sagittal arch deficiency
- Muscle spasm: R & L External Pterygoids, R Masseter
- Right Gonial angle more posterior
Orthogonal Radiographic Findings:
- Normal lordotic cervical curve with no osseous pathology.
- A-P view: Atlas Plane Angle is elevated 1 degree up on the right and skull is tipped to the left.
- Base Posterior Vertex: Atlas is rotated to the right.
Treatment:
- Correct the relapse factors by means of maxillary and mandibular ALF appliances.
- Orthogonal chiropractic adjustments.
Results:
- The right posterior unilateral crossbite was corrected in five visits with light forces
- Patient’s upper cervical and pelvic instabilities resolved.
- Fatigue level greatly reduced.
The purpose of this article is to draw the functional orthodontist’s attention to a comprehensive treatment approach for successfully correcting arch width deficiencies. An integration of osteopathic and chiropractic cranial concepts with the versatility of ALF orthopedics has provided a new treatment paradigm. For the first time in the history of orthodontics, a treatment concept is available that provides a means of diagnosing the factors which cause relapse. The ALF concept also provides an approach for the correction of unilateral posterior crossbite that will remain stable in over 95% of treated cases.

Fig.1 Pre-Treatment right posterior view: The maxillae was expanded by means of Crozat, however, the relapse indicators were not corrected and the case failed.

Fig. 2 Right posterior view: Crossbite corrected in five visits with light continuous forces generated by the ALF appliances. Speed of correction is due to proper sequencing of cranial releases by the ALF. Bilateral expansion would have expanded the left side since the right was internally rotated and locked. Relapse occurs because the normal left side will rebound since it was pushed beyond its envelop of adaptability. Any expansion in the right half will be very minimal with a bilateral expander and will also rebound due to the existing cranial distortion.

Fig. 3 Left posterior view: This half of the maxillae had abnormal development. The ALF appliances have the ability over appliances with mid-line screws to expand only the side which requires it. Expansion of the restricted left side can only be accomplished through releasing the cranium in proper sequence. The four indicators help establish the treatment priorities and sequencing.

Fig. 4 Pre-treatment model: The left half of the maxillae is in internal rotation and locked. Applying a bilateral force causes the left half to remain locked, resist expansion and cause over expansion of the right half. An illusion is created since the mandible will shift to the right in order to intercuspate with the upper arch.

Fig. 5 Post-Treatment Palatal view: Arch expansion was accomplished in five visits utilizing proper sequencing. Note anterior arch development compared to the pre-treatment model. The right half was able to expand once the cranial restrictions were released.

Fig. 6 Orthogonal Radiographic Analysis: evaluates a bisecting vertical line through the skull and spine to a 90 degree relation to the Atlas Horizontal Plane.
A-P View: Head is listing to left as a result of an Atlas subluxation.
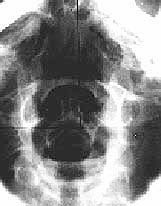
Fig. 7 Base Posterior Vertex: Atlas is rotated to the right. This view is used to evaluate for rotation of the Atlas.

Fig. 8 Lateral View: Used to evaluate the cervical lordotic curve, alignment of the spinous processes, frank pathology and determine the Atlas Plane Line angle.
References
- Ilana Brin, DMD, Yocheved Ben-Bassat, DMD, Yoei Biustein, DMD, Msc, Jacob Ehrlich. DMD, Nira Hochman, DMD, Yitzhak Marmary, DMD and Avinoam Yaffe, DMD. Skeletal and functional effects of treatment for unilateral posterior crossbite. Amer J of Orthodontics and Dentofacial Orthopedics Vol. 109: No. 2, Feb, 1996.
- Thilander B, Wahlund S, Lennartsson B. The effect of early interceptive treatment in children with posterior cross-bite. Eur J Orthod 1984; 6:25-34.
- Hermanson H, Kurol J, Ronnerman A. Treatment of unilateral posterior crossbite with quad helix and removable plates. A retrospective study. Eur J Orthod 1985; 7:97-102.
- Skieller V. Expansion of the midpalatal suture by removable plates, analysized by the implant method. Trans Eur Orthod Soc 1964:143-58.
