James E White, DO and Gregory A. Baldt, DC
High blood pressure is one of the major reasons patients see their physicians each year. Over 25 million patient visits were made to physicians for high blood pressure therapy in 1980, compared with only about 20 million patient visits for headaches last year.2
The chiropractor can play an important role in diagnosing and treating high blood pressure, using techniques of manipulating the cranium, face and total body.
High Blood Pressure
High blood pressure is a symptom of the disease known as “essential hypertension.” Many theories have been proposed to explain essential hypertension, but the actual cause of the disease is still unknown to the medical community at large. It has been billed as incurable, only controllable, with the axiom that every medical student learns, “Once a hypertensive, always a hypertensive.”
Hypertension gained notoriety in the 1940’s because it was believed to cause cardiac failures. Thus the name “silent killer” became inseparably linked to hypertension. Recent studies have shown that hypertension medications have not decreased the rate of cardiac failures, however.3
In the early 1950’s some osteopaths were treating hypertension with a combined cranial, facial and total-body approach to therapy. It was found that they could reduce the blood pressure this way for up to a month between treatments.4,5 With the advent and acceptance of diuretics and beta-blockers for hypertension therapy, the manipulative approach apparently has fallen to disuse. This is due to the ease which accompanies prescribing medication. It is obviously faster and easier to prescribe a medication to treat a symptom (high blood pressure), than it is to treat the actual biomechanical/structural cause of the disease (hypertension). This is not due to any increased effectiveness of medications on hypertension therapy; on the contrary, we have found that manipulation is often more effective than any single medication. Our patients preferred the manipulative approach, many having experienced unpleasant side effects from their medicinal therapies.
Hypertension
The diagnosis of essential hypertension in a patient is usually due to a blood pressure reading higher than (145/90). This elevated reading should be confirmed on at least three visits before diagnosing someone as hypertensive.
In cases of essential hypertension, usually both the systolic and diastolic pressure is elevated. When only the diastolic pressure is elevated without an accompanying rise in systolic pressure, it is “pulmonary hypertension.” This usually means that the filling pressure of the heart is too high, resulting from some type of a heart condition. Various heart tests are conducted, along with a different form of medicinal therapy. We shall confine the balance of the discussion to the more common type, or essential hypertension.
Hypertension was believed (by the medical community at large) to be related to several factors, especially the dietary intake of sodium and the amount of stress an individual experiences. The “conventional” approach to high blood pressure therapy uses two series of drugs. The first series usually used for mild high blood pressure are the diuretics, which work by removing the sodium ions (and generally the potassium ions as well) from the blood through the urine. The loss of too much potassium causes palpitations of the heart (patient feels their own heart pounding for no apparent reason) as well as dizziness.
It is interesting to note that in at least two independent studies the sodium link with hypertension was undercut.
“When 20,000 participants were subdivided into seven groups on the basis of their eating habits, the group with the smallest proportion of hypertensives (13.3%) was found to have a high sodium intake of 2.7 g daily; the group with the most hypertensives (22.3%) had a low sodium intake of 1.4 g/day,” said Melvin H. Freegly, PhD, of the University of Florida College of Medicine, Gainesville.
“The same inverse relationship between sodium intake and hypertension persisted when the sample group was reduced to 12,000 by eliminating participants who were aware of a hypertension problem and might have been cutting down on salt because of it,” said Dr. David A. McCarron, director of the hypertension program at Oregon Health Sciences University, Portland.
“Although different models have been proposed, the mechanism by which sodium may influence blood pressure remains hypothetical, and some investigators have said it probably is limited to a salt-sensitive group.”6
The second series of drugs generally used to treat hypertension are the beta-blockers. They are used when a person does not respond to diuretic therapy (high blood pressure remains elevated anyway), and act by “slowing down” the autonomic nervous system. Their mechanism is believed to block the receptors to segments of the spinal nervous system.
Many people using either diuretics or beta-blockers have “refractive hypertension,” meaning the medication is ineffective in controlling hypertension. Studies have shown that at least one-third of people will quit using hypertensive medications on their own, due to ineffectiveness or side effects.
Side Effects
There is a wide range of possible side effects of hypertensive medications. Below is a partial list of possible adverse reactions to a “typical” diuretic, Dyazide™ (Dyazide™ is a registered trademark of Smith, Kline & Frence Company):
Adverse Reactions: Muscle cramps, weakness, dizziness, headache, dry mouth; anaphylaxis, rash, urticaria, photosensitivity, purpura, other dermatological conditions; nausea and vomiting, diarrhea, constipation, other gastrointestinal disturbances; postural hypotension (may be aggravated by alcohol, barbiturates, or narcotics), Necrotizing vasculitis, paresthesias, icterus, pancreatitis, xanthopsia and respiratory distress including pneumonitis and pulmonary edema, transient blurred vision, sialadenitis, and vertigo have occurred with thiazides alone. Triamterene has been found in renal stones in association with other usual calculus components. Rare incidents of acute interstitial nephritis have been reported. Impotence has been reported in a few patients on Dyazide™, although a causal relationship has not been established.”7
Similarly, beta-blockers have possible adverse reactions as seen in the listing of a “typical” beta-blocker, such as Inderal™ (Inderal™, propanolol hydrochloride, is a registered trademark of Ayerst Laboratories)
- Cardiovascular: bradycardia, intensification of AV block, hypotension, arterial insufficiency, usually of the Raynaud type.
- Central Nervous System: light-headedness, mental depression manifested by insomnia, lassitude, weakness, fatigue, reversible mental depression progressing to catatonia, visual disturbances, hallucinations, short-term memory loss, emotional lability, slightly clouded sensorium, and decreased performance on neuropsychometrics.
- Gastrointestinal: nausea, vomiting, epigastric distress, abdominal cramping, diarrhea, constipation, mesenteric arteria thrombosis, ischemic colitis.
- Allergic: pharyngitis and agranulocytosis, erythematous rash, fever combined with aching and sore throat, laryngospasm and respiratory distress.
- Respiratory: bronchospasm.
- Hematologic: agranulocytosis, non-thrombocytopenic purpura, thrombocytopenic purpura.”8
Emotional lability means lack of emotional arousal, especially related to sexual intercourse.
Manipulative Approach to Therapy
The manipulative approach is a more holistic approach than the conventional medicinal therapies. The total-body is taken into consideration to determine the cause of the disease (hypertension) producing the symptom (high blood pressure). Unlike medicinal therapy, there are no adverse side effects. It has been the clinical experience of the author that the manipulative approach works in over 80% of cases, whereas medication apparently works less than 66% (at least 1/2, or 33%, stop their own medication because it does not work).
The manipulative approach is fairly straight-forward and simple. There are many variations of technique, but the underlying theme is to remove stress and relax the musculature of the head, neck and face. A common finding is the mandibular condyle is slightly recessed in the glenoid fossa of the temporal bone. This condition is sometimes referred to as “TMJ dysfunctional position.” The correction involves (for hypertension) “stopping the posterior glide of the mandible”9 by repositioning the jaw slightly forward, correcting any cranial faults, and repositioning the cranio facial bones as described by White and Baldt10. After correcting the faults, the blood pressure will usually decrease. Sometimes it decreases immediately, but may require up to 12 hours to return to a normal level.
For a prolonged effect, mouthpieces, correctly fitted, have proven very effective for maintaining the position of the craniofacial/TMJ mechanism and maintaining the effects of manipulation. Due to wear, the mouthpieces need to be checked (adjusted) periodically.
The mouthpieces are not a “cure” for hypertension. They are only an orthopedic appliance (like a heel lift or sacral support), used to help maintain the effect of the correct adjustment of the craniofacial/TMJ mechanism.
Comment
Ordinarily, most dentists try to “equilibrate” the occlusion (the way a person bites) or correct a “malocclusion” by pushing the mandible back into the “dental centric” position (most recessed position of the TMJ). This position causes the blood pressure to increase. Usually it does not increase instantaneously, but is diagnosed gradually, after several visits to the physician. Most patients and dentists do not make the correlation between the TMJ-recessed position and the new finding of hypertension in previously asymptomatic persons!
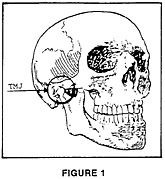
“When treating the TMJ, it is important to remember what the TMJ is. It is the articulation of the glenoid fossa of the temporal bone with the mandibular condyle. This articulation is near the external auditory meatus. The TMJ is not in the mouth. The correct positioning of the mandible to relieve the TMJ dysfunctional syndrome is primarily a structural and postural problem, necessitating direct intervention by a manual physician (chiropractor or osteopath). The TMJ dysfunctional syndrome is only secondarily related to the dentition. Let us re-emphasize the anatomical position of the TMJ: “The TMJ is not in the mouth!”11
Please refer to Figure 1, to recall the proper perspective of the location of the TMJ.
The systemic effects of only slightly altering the position of the TMJ are astounding. An increase of height of only 2 to 4 millimeters between the maxillary and mandibular molars on one side of the mouth can consistently produce a somatic dysfunction over the second cervical region on the opposite side of the body12. Similarly, a slightly different “balance” of a mouthpiece may produce, or relieve, specific headaches13. The correct positioning of the TMJ, craniofacial bones and fitting orthopedic appliance mouthpieces should necessarily be conducted by members of those professions familiar with the biomechanics and interrelationships of the human body.
The systemic effects relieved by the use of orthopedic mouthpieces or produced due to poorly fitted ones, such as high blood pressure, neck problems, headaches, specific somatic dysfunctions and eye pain, can easily be demonstrated by the physician skilled in systemic correction. These specific results, or cause-and-effect correlations, can be measured using thermography, X-ray, high blood pressure tests, and other diagnostic equipment.
Bibliography
- Family Practice News, November 1-14, 1982, “Over 25 Million Physician Visits for HT in 1980.”
- The Family Physician’s Compendium of Patient Information, section 16, “Headaches,” (Biomedical Information Corporation, New York: 1985).
- Family Practice News, January 15-31, 1986, “Says HT Therapy Hasn’t Cut Cardiac Failures,” p 18a.
- Northrup, Thomas L., DO, “Manipulative Therapy in Osteopathic Management of Hypertension,” The Journal of Osteopathy, September, 1950, pp 15-22.
- Northrup, Thomas L., DO “Manipulative Management of Hypertension,” Journal of the American Osteopathic Association, August, 1961, pp 973-978.
- Family Practice News, November 1-14, 1982, “Epidemiologic Study Undercuts Sodium Link with Hypertension.”
- Dyazide advertisement, Journal of the American Osteopathic Association, September, 1984, back cover.
- Ibid., pl/8.
- Odaffer, R.G., DO, and James E. White, DO, “Hypertension,” Basal Facts, Spring, 1980, pp 23-25.
- White, James E., DO, and Greg Baldt, DC. New Cranial: Direct Craniofacial Technique, (Pain Control Systems, Arizona: 1986) pp 47-54.
- Ibid., pp 15, 16.
- White, William K., James E. White, DO, and Greg Baldt, DC, “The Relation of the Craniofacial Bones to Specific Somatic Dysfunctions: A Clinical Study of the Effects of Manipulation,” Journal of the American Osteopathic Association, September, 1984, pp 603-604.
- White, James E., DO, Dentosomatics; (Copyright, Farmington, New Mexico: 1981) pp 15-18, 39.
