Dental / Dermatologic Connection
This case clearly links a distant area that was directly affected by a dental focal infection. Such infected teeth produce thiol ethers, which are extremely poisonous compounds that have a sulfhydryl group (SH). These sulfur groups bind heavy metals like mercury. Many patients suffer systemic medical problems that have their origin from infected teeth and unfortunately most dentists and physicians will miss the diagnosis. Such infections have the potential for causing rheumatic joint pain, chronic fatigue, irritable bowel syndrome (IBS), skin rashes, chronic sore throat, swollen lymph nodes, low-grade fever and even cancer. Many times patients who have cancer that does not respond to treatment have dental infections, which prevent the cancer from resolving. Reversing Cancer, soon to be published, goes into greater detail on this subject.
As far back as the 1930’s dentists were aware of the impact that infected teeth played on the systemic health of the patient. Symptomless foci (infected teeth or areas in the jawbone) were and are still difficult to diagnose with conventional means. Visual inspection most often reveals healthy looking structures: teeth, gums and even x-rays reveal no pathology. In addition, patients often have mild to no pressing complaints of pain, sensitivity, bleeding gums or tooth mobility in the immediate vicinity of the problem area. The bacteria isolated from symptomless foci, while having high specific virulence, usually have only a low general virulence and hence are incapable of causing acute symptoms at the primary site.
Radiographically negative teeth are frequently considered sterile and harmless and are allowed to remain despite the fact that they have been shown by special diagnostic methods to be infected by streptococci or other organisms. One cannot see bacteria at the apexes of these involved teeth in the x-ray. The infection present may or may not cause absorption of bone. According to Edward C. Rosenow, MD, head bacteriologist of the Mayo Clinic in the 1940’s, negative pulpless teeth in his experience were more specifically virulent than those isolated from radiographically positive teeth (teeth with abscesses).
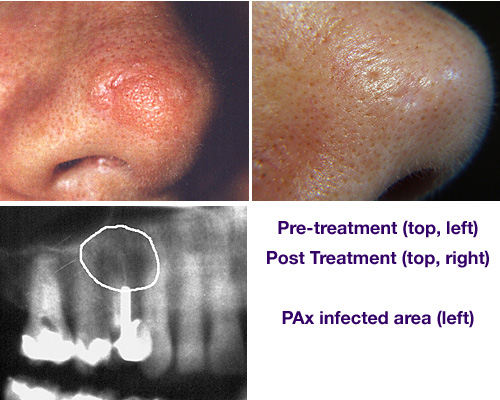
P.M. is a 55-year-old Caucasian female who had a raised lesion (similar in appearance to a basal cell carcinoma: slow growing cancer) on the right side of her nose just above her nostril. This lesion persisted for more than one year. Evaluation by a dermatologist established a high level of suspicion of being a cancerous lesion. It was recommended that the lesion be surgically removed and biopsied. About the time of this medical evaluation, the patient was examined and evaluated for dental/somatic complaints of chronic headaches, neck and low back pain. Testing uncovered the presence of a streptococcal infection and jaw osteitis (inflammation of the jawbone) in the region of the upper right first bicuspid tooth. Sanum remedies from Germany were tested against the strep infection. The appropriate homeopathic remedies were injected into the jawbone that surrounded the involved tooth. Post treatment witnessed a reduction in the size and elevation of the nose lesion for a three-week period. Because orthodontics was planned the tooth was needed as an anchor and therefore not removed during treatment. Periodic injections were performed to keep the nose lesion under control. Upon completion of dental treatment, the infected upper right bicuspid tooth was extracted and biopsied. The infected bone lining the socket was drilled out and the surgical site was packed with gelfoam (a sponge that reabsorbs) saturated with the homeopathic remedies. The site healed uneventfully. The biopsy report confirmed the presence of chronically inflamed necrotic (dead) bone with an apical granuloma (area of soft tissue that could not heal due to dead tissue and inflammation). Also present was necrotic or dead pulpal tissue in the apical canal (area at the end of the root).
Dermotologist recommended surgical removal of a raised lesion on patient’s nose, in effect, treating the symptom. Dr. Smith discovered and treated the “cause,” which involved, among other things, a “hidden” streptococcal infection. Surgery avoided—case closed.

STAY INFORMED
Big tech and mainstream media try to suppress the powerful information I have to share. Subscribe here to stay informed!