Dr. Hans Selye
International Institute of Stress
University of Montreal
Montreal, Quebec, Canada
The Nature of Stress was submitted to Dr. Fonder shortly before Selye’s death. Dr. Fonder knew him well having been invited by Selye to share his lecture platform on several occasions.
This treatise is presented as prepared by Hans Selye as if he is still living, which indeed he is through his monumental works, for Dr. Stress, as he was occasionally entitled, will live forever since so many believe that Hans Selye is the foremost medical researcher of the 20th century.
About the Author: Dr. Hans Selye is without question one of the great pioneers of medicine. His famous and revolutionary concept of stress opened countless avenues of treatment through the discovery that hormones participate in the development of many degenerative diseases, including coronary thrombosis, brain hemorrhage, hardening of the arteries, high blood pressure and kidney failure, arthritis, peptic ulcers and even cancer. At present, most of his research is concerned with formulating a code of behavior based on the laws governing the body’s stress resistance in dealing with personal, interpersonal and group problems.
Dr. Selye has served since 1945 as professor and Director of the Institute of Experimental Medicine and Surgery at the University of Montreal. Now he is President of the International Institute of Stress, founded by him in 1976 at the University of Montreal.
Born in Vienna in 1907, he studied in Prague, Paris, and Rome. He received his medical degree and his Ph.D. (chemistry) from the German University in Prague, and his D.Sc. at McGill University in Montreal. He is the author of 38 volumes and more than 1600 technical articles. In addition to his doctorates he holds 20 honorary degrees from universities around the world. He is a Fellow of the Royal Society of Canada and an Honorary Fellow of 68 other scientific societies. A recipient of numerous honorary citizenships, he counts among his medals the Starr Medal (highest distinction of the Canadian Medical Association); the Prix de I’Oeuvre Scientifique (highest award of the Canadian Association of Frenchspeaking Physicians); the Killam Scholarship (highest award of the Canada Council); the International Kittay Award (top prize in psychiatry); the American Academy of Achievement’s Golden Plate Award,- and the 1977 Canadian Authors Association Literary Award for nonfiction. He has, in addition, been made a Companion of the Order of Canada (the highest decoration awarded by his country).
When I wrote the first paper on the stress syndrome in 1936, 1 tried to demonstrate that stress is not a vague concept, somehow related to the decline in the influence of traditional codes of behavior, dissatisfaction with the world, or the rising cost of living, but rather that it is clearly a definable biological and medical phenomenon whose mechanisms can be objectively identified and with which we can cope much better once we know how to handle it.
Since then, a great deal of progress has been made in identifying the mechanisms of stress-induced bodily responses. And during recent years, considerable knowledge has been acquired about comprehending and controlling stress through scientific techniques. The results are of immense practical value for further improving the understanding of stress mechanisms by scientists, and for the treatment of certain stress-induced derangements by competent physicians.
Yet today, though everyone talks about stress, only a few people know exactly what it is. It is hard to read a newspaper or watch a television program without hearing about stress, and literally hundreds of people now lecture and write about it. They are ever ready to give advice, usually based on the teachings of an Eastern guru or Western “stressologist” – advice that works well provided that one has absolute faith in the master’s divine infallibility. Far be it from me to suggest that these people have nothing to offer, but in the absence of a clear concept of exactly what stress is, one is not likely to find it easy to maintain faith should difficulties crop up. Besides, in the modern world there are so many prophets around trying to convince us that a desire to adopt their faith is enough.
When confusions and arguments about stress – indeed about any concept – start to prove a barrier to communication and progress, it is always best to revert to the undisputed facts, the original observations that gave rise to the field. Accordingly, let us proceed to a discussion of the nature of stress.
What stress is not
The word stress has been used so loosely, and so many confusing definitions of it have been formulated, that I think it will be best to start by clearly stating what it is not. Contrary to current popular or medical opinion:
- Stress is not nervous tension. Stress reactions do occur in lower animals and even in plants, which have no nervous system. The general manifestations of an alarm reaction can be induced by mechanically damaging a denervated limb. Indeed, stress can be produced under deep anesthesia in patients who are unconscious, and even in cell cultures grown outside the body.
- Stress is not an emergency discharge of hormones from the adrenal medulla. An adrenaline discharge is frequently seen in acute stress affecting the whole body, but it plays no conspicuous role in generalized inflammatory diseases (arthritis, tuberculosis) although they can also produce considerable stress. Nor does an adrenaline discharge play any role in “local stress” reactions, limited to directly injured regions of the body.
- Stress is not that which causes a secretion by the adrenal cortex of its hormones (the corticoids). ACTH, the adrenal-stimulating pituitary hormone, can discharge these hormones without producing any evidence of stress.
- Stress is not the nonspecific result of damage only. Normal and even pleasant activities – a game of tennis or a passionate kiss – can produce considerable stress without causing conspicuous damage.
- Stress Is not the deviation from homeostasis, the steady state of the body. Any specific biologic function, e.g., the perception of sound or light, the contraction of a muscle, eventually causes marked deviations from the normal resting state in the active organs. This is undoubtedly associated with some local demand for increased vital activity, but it can cause only “local stress” and even this does not necessarily parallel the intensity of the specific activity.
- Stress is not that which causes an alarm reaction. The stressor does that, not stress itself.
- Stress is not identical with the alarm reaction or with the G.A.S. as a whole. These are characterized by certain measurable organ changes which are caused by stress.
- Stress itself is not a nonspecific reaction. The pattern of the stress reaction is very specific: it affects certain organs (e.g., the adrenal, the thymus, the gastrointestinal tract) in a highly selective manner.
- Stress is not a reaction to a specific thing. The stress response can be produced by virtually any agent.
- Stress is not necessarily undesirable. It all depends on how you take it. The stress of failure, humiliation, or infection is detrimental; but that of exhilarating, creative, successful work is beneficial. The stress reaction, like energy consumption, may have good or bad effects.
- Stress cannot and should not be avoided. Everybody is always under some degree of stress. Even while quietly asleep our heart must continue to beat, our lungs to breathe, and even our brain works in the form of dreams. Stress can be avoided only by dying. The statement “He is under stress” is just as meaningless as “He is running a temperature. ” What we actually refer to by means of such phrases is an excess of stress or of body temperature.
If we consider these points, we may easily be led to conclude that stress cannot be defined, and that perhaps the concept itself is just not sufficiently clear to serve as the object of scientific study.
Nevertheless, stress has a very clear, tangible form. Countless people have actually suffered or benefited from it. Stress is very real and concrete indeed, and is manifested in precisely measurable changes within the body. So before we proceed to a formal definition of the nature of stress, we will describe these manifestations.
What stress is
Mechanism. The workings of stress are extremely complex (see Figure below). Apart from specific stimuli, which need not be discussed here, the first effect of any, agent or demand made upon the body – be it running up a flight of stairs, dealing with a viral infection, or performing a dance – is to produce a nonspecific stimulus (the agent’s “stressor effect”.) This may be a nervous impulse, a chemical substance or lack of an indispensable metabolic factor; it is referred to simply as the “first mediator,” because we know nothing about its nature. We are not even certain that it has to be an excess or deficiency of any particular substance; it is possible that various derangements of homeostasis can activate the stress mechanism.
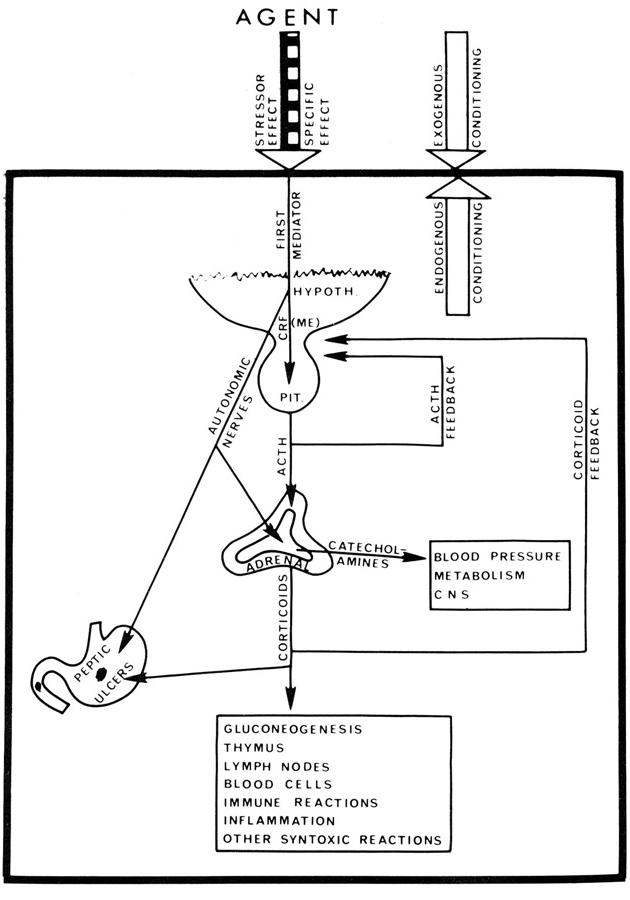
Although we have still to identify the first mediator(s), we do know that eventually stress acts upon the hypothalamus and particularly upon the median eminence (ME). This action appears largely to be mediated through or modified by nervous stimuli coming from the cerebral cortex, the reticular formation and the limbic system (especially the hippocampus and amygdala). The incoming nervous stimuli reach certain neuroendocrine cells, most of which are located in the ME. These act as “transducers, ” transforming nervous signals into a humoral messenger, the corticotrophic hormone releasing factor (CRF), which can be demonstrated histochemically in the ME region and can also be extracted from it. Oddly enough, the posterior pituitary contains the highest concentration of CRF, and it has been isolated from this source in pure form, thus permitting the determination of its chemical formula as a polypeptide which subsequently was synthesized. Yet we have no conclusive proof that the CRF-active material extracted from the hypothalamus is identical with that obtained from the posterior lobe since only the structure of the latter has been definitely ascertained. Although vasopressin (antidiuritic hormone) possesses considerable CRF activity it is not identical with CRF; this has been shown by the welldocumented differences in their chemical structure and physiologic activity.
CRF reaches the anterior lobe through the hypothalamo-hypophyseal portal system that originates in the ME region within a network of capillaries into which CRF is discharged by the local neuroendocrine cells. It is then carried down through the larger veins of the pituitary stalk to a second capillary plexus in the pituitary.
The hypothalamus does not stimulate the adrenocorticotrophic hormone (ACTH) secretion of the anterior lobe through nervous pathways descending in the pituitary stalk but rather through blood-borne substances carried by way of the portal veins. That is why transection of the stalk inhibits the ACTH secretion only before vascular connections between the hypothalamus and the gland are reestablished; if regeneration of these vessels is prevented by interposing a plate between the cut ends of the stalk, this pathway is permanently blocked.
Both in vivo and in vitro experiments have proven that CRF elicits a discharge of ATCH from the adenohypophysis into the general circulation. Upon reaching the adrenal cortex, it causes secretion of corticoids, mainly glucocorticoids such as cartisol or corticosterone. These induce glyconeogenesis, thereby supplying a readily-available source of energy for the adaptive reactions necessary to meet the demands faced by the body. In addition, they facilitate various other enzymatically regulated adaptive metabolic responses and suppress immune reactions as well as inflammation, assisting the body to coexist with potential pathogens (syntoxic reactions). Furthermore, the glucocorticoids are responsible for the thymicolymphatic involution, eosinopenia and lymphopenia characteristic of acute stress. Curiously, glucocorticoids are needed for the acquisition of adaptation primarily during the alarm reaction, but not so much to maintain the adjustment during the stage of resistance. ACTH plays a comparatively minor role in the secretion of mineralocorticoids, such as aldosterone, which is regulated mainly by the renin-hypertension system and the blood electrolytes, whose homeostasis is in turn influenced by them.
This chain of events is cybernetically controlled by several biofeedback mechanisms. Whether an excess of CRF can inhibit its own endogenous secretion is still doubtful because its lifespan in the circulating blood is very short. On the other hand, there is definite proof of an ACTH feedback (short-loop feedback) by a surplus of the hormone, which returns to the hypothalamo-pituitary system and inhibits further ACTH production. We have even more evidence to substantiate the existence of a corticoid feedback mechanism (long-loop feedback) in that a high blood corticoid level similarly inhibits ACTH secretion. It is still not quite clear to what extent these feedbacks act upon the neuroendocrine cells of the hypothalamus, the adenohypophysis or both. (Hence, in the Figure the corresponding arrowheads merely point towards the hypothalamo-hypophyseal region in general, without specifying exactly where their target areas are situated.)
Another major pathway involved in the stress mechanism is carried through the catecholamines liberated under the influence of an acetylcholine discharge, at autonomic nerve endings and in the adrenal medulla. The chromaffin cells of the latter secrete mainly epinephrine, which is of considerable value in that it stimulates mechanisms of general utility to meet various demands for adaptation. Thus it provides readily available sources of energy by forming glucose from glycogen depots and free fatty acids from the triglyceride stores of adipose tissue; it also quickens the pulse, raises the blood pressure to improve circulation into the musculature, and stimulates the CNS. In addition, epinephrine accelerates blood coagulation and thereby protects against excessive hemorrhage should wounds be sustained in conflicts. All of this is helpful in meeting the demands, whether they call for fight or flight.
At this point it will be helpful to discuss two apparent objections to accepting the concept of a single stereotyped response to stress:
- Qualitatively different agents of equal toxicity or stressor potency do not necessarily elicit exactly the same reactions in different people.
- Even the same degree of stress, induced by the same agent, may produce different effects and even lesions in different individuals.
- The effects specific to any given agent usually modify the effects and manifestations of the general stress syndrome. (thus, it took many years to recognize and prove the existence of the latter.)
- The fact that the state of stress, even if due to the same agent, can cause different effects in different individuals, has been traced to “conditioning factors” that can selectively enhance or inhibit one or the other stress effect. This conditioning may be endogenous (genetic predisposition, age or sex) or exogenous (treatment with certain hormones, drugs, or dietary factors.) (See Figure.) Under the influence of such conditioning factors, a normally well-tolerated degree of stress can even become pathogenic, selectively affecting those parts of the body that are particularly sensitized both by those conditioning factors and by the specific effects of the eliciting agent, just as physical tensions of equal strength in different chains will break the particular link that is the weakest as a result of internal or external factors.
The foregoing processes are the principal ones involved in the stress reaction, but by no means the only ones. As well, the level of STH, the growth hormone, may rise, and changes in the output of thyroid hormones of the ovary or testis may take place.
Stressors. The agents or demands that evoke this coordinated response which I have designated 11 stress” are referred to, quite naturally, as stressors; and of course something is a stressor to the same degree that it calls forth the syndrome.
When the stressor in question is some organism or substance foreign to the body, the curative process resulting from the stress reaction can take either of two forms, according to whether the pathogen causes trouble directly or indirectly. Direct pathogens cause disease irrespective of our body’s reaction, whereas indirect pathogens produce damage only through the exaggerated and purposeless defensive responses they provoke. If a patient accidentally exposes his hand to a strong acid, alkali, or boiling water, damage will occur irrespective of his reactions. Because all these are direct pathogens; they would cause damage even to the body of a dead man who obviously could not put up any vital defense reactions. On the other hand, most common inflammatory irritants, including allergens, are essentially indirect pathogens, which do not themselves cause disease, but are damaging only by stimulating an inopportune and harmful fight against what is innocuous.
During evolution, immunologic reactions which lead to destruction of microbes, grafts, and other foreign tissues undoubtedly developed as useful defensive mechanisms against potentially dangerous foreign materials. However, when – as in the case of many allergens, heart transplants, etc. – the attack against the “foreign” agent is unnecessary or even harmful, man can improve upon the wisdom of Nature by suppressing this hostility. Nevertheless, when the aggressor is dangerous, the defensive reaction should not be suppressed but, if possible, increased above the normal level, which can be done, for ex ample, by catatoxic substances that carry the chemical message to the tissues to destroy the invaders even more actively than would normally be the case.
However, stressors are not exclusively physical in nature. Emotions, e.g., love, hate, joy, anger, challenge and fear, also call forth the changes characteristic of the stress syndrome.
Stress and disease. In general, the hormonal responses outlined above aid adaptation to environmental change or stimuli; but they are sometimes the cause of disease, especially if the state of stress is prolonged or intense. In this latter case, the body goes through the three stages of what I call the “general adaptation syndrome” (G.A.S.). The first is the alarm reaction, characterized by the changes above described. Of course, if the stressor (stress-producing agent) is so severe that continued exposure is incompatible with life, the organism will die within a few hours during this stage; otherwise, a stage of adaptation of resistance will ensue, since no organism can be maintained continuously in a state of alarm. The adaptive stage is characterized by the vanishing or diminishing of the initial symptoms, since the body has achieved optimal adaptation. After still more prolonged exposure to the stressor, however, this acquired adaptation is lost and a third stage of exhaustion is entered into, which, unless the organism receives emergency aid from some outside source, leads to death. Apparently, the adaptability of an organism is finite.
An important instance of prolonged stress is that brought about by various dental problems such as tooth loss and the resultant malocclusion, muscular imbalances and ensuing unrelenting muscle tensions which create both physical and psychological demands. These conditions are often left untreated for years and even decades, and it is easy to see how trouble in this area might lead not only to local wear and tear but also to general, systemic stress, which in turn may create other problems or intensify the original ones. As Dr. Fonder says, describing the ailments associated with malocclusion: “It is interesting to note the routine interplay of the autonomic nervous system in the symptomotology throughout this total person when analysing the data on each patient. Also of interest is the routine picture of endocrine gland disturbance that Selye [The Stress of Life, New York, McGraw-Hill, Inc., 19561 so ably depicted in the General Adaptation Syndrome brought on by any Stress to the body.”‘
Definition. Let us see now whether the following definition will fit all our facts:
Stress is the state manifested by a specific syndrome which consists of all the nonspecifically-induced changes within a biologic system. Thus, stress has its own characteristic form and composition, but no particular cause. The elements of its form are the visible changes due to stress, which are addictive indicators expressing the sum of all the different adjustments that are going on in the body at any time.
The above is essentially an “operational definition”; it tells what must be done to produce and recognize stress. A state can be recognized only by its manifestations; you have to observe a great many living beings exposed to a variety of agents before you can see the shape of stress as such. Those changes which are induced by only one or the other agent must first be rejected; if you then take what is left – that which is induced by many agents – you have uncovered stress itself.
For simplicity’s sake we have attempted to state the essence of this concept in the following, less formal terms:
Stress is the nonspecific response of the body to any demand, whether is is caused by, or results in, pleasant or unpleasant conditions. Stress as such, like temperature as such, is all-inclusive, embodying both the positive and the negative aspects of these concepts.
Within the general concept of stress, however, we must differentiate between distress (from the Latin dis = bad, as in dissonance, disagreement), and eustress (from the Greek eu = good, as in euphonia, euphoria). During both eustress and distress the body undergoes virtually the same nonspecific responses to the various positive or negative stimuli acting upon it. However, the fact that eustress causes much less damage than distress graphically demonstrates that it is “how you take it” that determines, ultimately, whether you can adapt successfully to change.
The general adaptation syndrome
Definition. While stress is reflected by the sum of the nonspecific changes as they develop throughout time during continued exposure to a stressor, the G.A.S. encompasses all nonspecific changes as they occur during continued exposure to a stressor. One is a snapshot, the other a motion picture of the response to demands.
Thus, the G.A.S. may be defined as the manifestation of stress in the whole body, as they develop in time. As we have seen, a fully-developed G.A.S. consists of three stages: the alarm reaction, the stage of resistance, and the stage of exhaustion. Yet it is not necessary for all three stages to develop before we can speak of G.A.S. Only the most severe stress leads rapidly to the stage of exhaustion and death. Most of the physical or mental exertions, infections, and other stressors, which act upon us during a limited period, produce changes corresponding only to the first and second stages: at first they may upset and alarm us, but then we adapt to them.
Normally, in the course of our lives, we go through these first two stages many, many times. Otherwise we could never become adapted to all the activities and demands which are man’s lot. Even the stage of exhaustion does not always need to be irreversible and complete, as long as it affects only parts of the body. For instance, running produces a stress situation, mainly in our muscles and cardiovascular system. To cope with this, we first have to limber up and get these organs ready for the task at hand; then for a while we will be at the height of efficiency in running, but eventually exhaustion will set in. This could be compared with an alarm reaction, a stage of resistance, and a stage of exhaustion, all limited primarily to the muscular and cardiovascular system. But such exhaustion is reversible; after a good rest we will be back to normal.
Most human activities go through three stages analogous to those of the G.A.S.: we first have to get into the swing of things, then we get pretty good at them, but finally we tire and lose our acquired efficiency. This triphasic evolution of adaptation is quite characteristic also of all bodily activities, including those that only the physician can fully appraise; for instance, of inflammation. If some virulent microbes get under the skin, they first cause what we call acute inflammation (reddening, swelling, pain); then follows chronic inflammation (ripening of a boil or abcess); and finally an exhaustion of tissue resistance takes place, which permits the inflamed, purulent fluid to be evacuated (breaking through of an abcess).
The diseases of adaptation. Many maladies are due not so much to what happens to us as to our inability to adapt, and they have therefore been called “diseases of adaptation. ” The most common of such diseases are peptic ulcers in the stomach and upper intestine, high blood pressure, heart accidents, and nervous disturbances. Of course, any event makes demands upon us and, hence, causes some stress, but it is only people who cannot cope, either because of innate defects or lack of knowledge, who develop stress diseases.
Yet this is a relative concept. No malady is just a disease of adaptation. Nor are there any disease producers which can be so perfectly handled by the organism that maladaptation plays no part in their effects upon the body. Such agents would not produce disease. This haziness in its delimitation does not interfere with the practical utility of our concept. We must put up with the same lack of precision whenever we have to classify any other kind of disease. There is no pure heart disease, in which all other organs remain perfectly undisturbed, nor can we ever speak of a pure kidney disease or a pure nervous disease in this sense.
The concept of adaptation energy. The selective exhaustion of muscles, eyes, or inflamed tissue all represent final stages in local adaptation syndromes (L.A.S.) only. Several of these may develop simultaneously in various parts of the body; in proportion to their intensity and extent, they can activate the G.A.S. mechanism. It is when the whole organism is exhausted – through senility at the end of a normal life-span, or through the accelerated aging caused by stress – that we enter into the (fatal) stage of exhaustion of the G.A.S.
Apparently, we have hidden reserves of adaptability, or adaptation energy, in ourselves throughout the body. As soon as local stress consumes the most readily accessible local reserves, local exhaustion sets in and activity in the strained part must stop. This is an important protective mechanism because, during the period of rest thus enforced, more adaptation energy can be made available, either from less readily accessible local stores or from reserves in other parts of the body. Only when all of our adaptability is used up will irreversible, general exhaustion and death follow.
Adaptation energy and a natural code of behavior
There seem to be close interrelations between the G.A.S. and aging. We have already mentioned that several local adaptation syndromes may develop consecutively or even simultaneously in the same individual. People can get used to a number of things (cold, heavy muscular work, worries), which at first had a very alarming effect; yet, upon prolonged exposure, sooner or later all resistance breaks down and exhaustion sets in. The term “adaptation energy” has been coined for that which is consumed during continued adaptive work, to indicate that it is something different from the caloric energy we receive from food; but this is only a name, and even now we still have no precise concept of what this energy might be. Further research along these lines would seem to hold great promise, since we appear to touch upon the fundamentals of fastigue and aging.
Seemingly, each individual inherits a certain amount of adaptation energy, the magnitude of which is determined by his genetic background, his parents. He can draw upon this capital thriftily for a long but monotonously uneventful existence, or he can spend it lavishly in the course of a stressful, intense, but perhaps more colorful and exciting life. In any case, there is just so much of it, and he must budget accordingly.
How can we, as individuals, best manage our limited store of this energy? Surely scientists have found enough evidence to justify trying to develop the fundamentals of a code of behavior based only on the laws of Nature, though we may need much more scientific work to learn how to apply them in our daily life and to make them easily understandable.
In the light of what my own laboratory and clinical study of somatic diseases has taught me concerning stress, I have tried to arrive at a code of ethics based not on the strictures and traditions of society, inspiration, or blind faith in the infallibility of a particular prophet, religious leader or political doctrine, but on the scientifically verifiable laws that govern the body’s reactions in maintaining homeostasis and living in satisfying equilibrium with its environment. By means of such a code, we can adjust our personal reactions to enjoy fully the eustress of success and accomplishment without suffering the distress commonly generated by frustrating friction and purposeless, aggressive behavior against our surroundings.
It is a biologic fact that man – like the lower animals – must fight and work for some goal that he considers worthwhile. We must use our innate capacities to enjoy the eustress of fulfillment. Only through effort, often aggressive, egoistic effort, can we maintain our fitness and assure our homeostatic equilibrium with both the social and the inanimate world. To achieve this state, our activities must earn lasting results; the fruits of work must be cumulative and must provide a capital gain to meet future needs. To succeed, we have to accept the scientifically established fact that man has an inescapable natural urge to work egoistically for things that can be stored to strengthen his homeostasis in the unpredictable situations with which life may confront him.
We should not combat or be ashamed of these instincts. We can do nothing about having been built to work, and it is primarily for our own good. Organs that are not used (muscles, bones, even the brain) undergo inactivity atrophy, and every living being looks out first of all for itself. Neither should we feel guilty because we work for treasures that can be stored to ensure our future homeostasis. Hoarding is a vitally important biologic instinct that we share with animals such as ants, bees, squirrels and beavers. In man, the urge first manifests itself when children start to gather match boxes, shells or stickers; it continues when adults collect stamps or coins. Such a universal Dr cannot be an artificial, indoctrinated tradition.
On the other hand, there is no example in Nature of a creature guided exclusively by altruism and the desire to protect others. In fact, a code of universal altruism would be highly immoral, since it would expect others to look out for us more than themselves. Of course, “Love thy neighbor as thyself” is a command full of wisdom; but, as originally expressed, it is incompatible with biologic laws; no one needs to develop an inferiority complex if he cannot love all his fellow men on command.
What are the ingredients of a code of ethics that accepts egoism and working to hoard personal capital as morally correct? After four decades of clinical and laboratory research, I would summarize the most important principles briefly as follows:
- Find you own stress level – the speed at which you can run toward your own goal. Make sure that both the stress level and the goal are really your own, an not imposed upon you by society, for only you yourself can know what you want and how fast you can accomplish it. There is no point in forcing a turtle to run like a racehorse or in preventing a racehorse from running faster than a turtle because of some “moral obligation.” The same is true of people.
- Be an altruistic egoist. Do not try to supress the natural instinct of all living beings to look after themselves first. Yet the wish to be of some use, to do some good to others, is also natural. We are social beings, and everybody wants somehow to earn respect and gratitude. You must be useful to others. This gives you the greatest degree of safety, because no one wishes to destroy a person who is useful.
- Earn thy neighbor’s love. This is a contemporary modification of the maxim “Love thy neighbor as thyself.” It recognizes that not all neighbors are lovable and that it is impossible to love on command.
Perhaps two short lines can encapsulate what I have discovered from all my thought and research:
Fight for your highest attainable aim,
But do not put up resistance in vain.
So far as possible, I myself have followed this philosophy, and it has made my life a happy one. Frankly, in looking back, I realize that I have not always succeeded to perfection, but this has been due to my own shortcomings, not those of the philosophy. As I have often said. The builder of the best racing car is not necessarily its best Drr.
Notes
- Undoubtedly, in man, with his highly developed central nervous system (CNS), emotional arousal is one of the most frequent activators. Yet it cannot be regarded as the only factor, since typical stress reactions can occur in patients exposed to muscle fatigue, trauma, hemorrhage, etc. while under deep anesthesia. Indeed anesthetics themselves are commonly used in experimental medicine to produce stress, and 11 stress of anesthesia” is a serious problem in clinical surgery.
- A.C. Fonder, “Malocclusion as it relates to general health,” Illinois Dent. J. 34 (5) (May 1965): pp.292-302.
Bibliography
- Appley, Mortimer H., and Trumball, Richard. Psychological Stress: issues in research. New York: Appleton-Century-Crofts, 1967.
- Klausner, Samuel Z. Why Man Takes Chances. Garden City (New York): Anchor Books, Doubleday, 1968
- Mason, J.W. A historical view of the stress field. Part 1. J. hum. Stress 1(1): 6-12 (1975).
- Mason, J.W. A historical view of the stress field. Part 11 J. hum. Stress 1 (2): 22-36 (1975).
- Selye, H. Confusion and controversy in the stress field. J. hum. Stress 1 (2): 37-44 (1975) (Answer to the preceding articles.)
- Selye, H. From Dream to Discovery. New York: McGraw-Hill, 1964.
- Selye, H. Hormones and Resistance. BerlinHeidelberg-New York: Springer-Verlag, 1971.
- Selye, H. In Vivo. The Case for supramolecular biology. New York: Liveright, 1967.
- Selye, H. The Story of the Adaptation Syndrome. Montreal: Acta, Inc., 1952.
- Selye, H. Stress in Health and Disease. Reading (Mass.): Butterworths, 1976.
- Fonder, A.C. The Dental Physician. The University Press, Blacksburg, VA., 1977.
- Selye, H. The Stress of Life. New York: McGrawHill, 1956. Rev. ed. 1976.
- Selye, H. Stress without Distress. New York: Lippencott, 1974.
- Selye, H. A Syndrome produced by diverse nocuous agents. Nature 138: 32 (1936).
- Fonder, A.C. Malocclusion as it relates to general health. Illinois Dental Journal 34 (5) (May 1965): pp. 292-302.
