Dental / Sciatic Pain Connection
Patients with relentless sciatic pain have a tremendous burden to bear. Living with any kind of pain is not pleasant but sciatic pain can be especially disabling. A main symptom is sciatic neuralgia, or pain starting from the buttocks and shooting down the back of the leg and sometimes into different portions of the lower leg. The sciatic nerve runs right through the belly of the piriformis muscle and if the piriformis muscle contracts from being overused, the sciatic nerve now becomes entrapped, producing pain, tingling and numbness. Siciatic pain can come from many different sources (herniated disc, pronated foot, upper cervical dysfunction) however, one origin is not too well known- dental/cranial distortion.
The Sacro-Occipital Technique developed by Major B. DeJarnette, DC and Applied Kinesiology developed by George Goodheart, DC are two chiropractic concepts that provide a global approach designed to treat the body more comprehensively. The functional connection lies in the dural tube that connects the cranio dental complex, spine and sacral/pelvic complex. The so-called “slinky” effect clearly describes this system. Two applied kinesiologists, Drs. Herbert Anderson and Carl Ferrari, recognized and demonstrated that there is a direct muscle interlink between the chewing muscles and the muscles, which help stabilize the pelvis (gluteus medius, obturator internus, quadratus lumborium, psoas and leg adductors). Another connecting link stems from the Lovett Brother relationship, which relates specific bone interlinks between the skull and pelvic complex. Distortions from either end will reflect upward or downward and the structures in between will compensate.
Norma B. suffered with constant sciatic pain for three years. Neurologists, chiropractors, physical therapists and medical doctors could not resolve her pain. Norma’s quality of life was non-existent. At her daughter’s request, Norma made an evaluation appointment. Norma presented a primary cranial/dental distortion accompanied by primary pronation of the feet. A severe scoliosis was also present. When tested, her left piriformis muscle was weak. Interestingly, when her cranium was rebalanced and a “shim” placed on one tooth to support her skull alignment, the left piriformis muscle immediately strengthened. In 90 minutes of treatment, Norma got up from the dental chair and in total disbelief stated that her sciatic pain was totally gone. The key to successful treatment was the fact that the underlying structural imbalances were diagnosed and properly treated.
Figure 1.

A ‘shim” was placed on the lower right second molar to level the cranial bone alignment and remove the strain from the dural memebrane tube.
Figure 2.

A minor occlusal interference was removed from the lower left second molar. This neurological abnormality of the bite was a factor in causing the weakness of the left piriformis muscle.
Figure 3.

Norma had bilateral pronation. The right foot pronation was worse than the left. Norma’s therapist placed a 6mm proprioceptive stimulator in both shoes to correct the structural imbalance.
Figure 4.
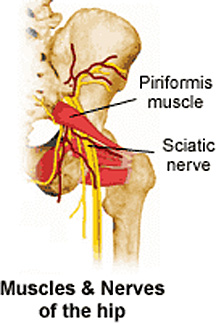
The function of the piriformis muscle can be directly affected by a malocclusion and/or mechanical interference in the bite. The piriformis muscle is attached to the scarum, which is directly influenced by the dural tube.
The functional connection lies in the dural tube that connects the cranio dental complex, spine and sacral/pelvic complex.
FREE PRESENTATION
Download the slides from Dr. Smith's presentation on the Dental Whole Body Connection in Ontario on October 25, 2024.
A comprehensive seminar to awaken you to the potential dangers of dental treatments.

STAY INFORMED
Big tech and mainstream media try to suppress the powerful information I have to share. Subscribe here to stay informed!